American Rescue Plan Continued
It was recently announced that The American Rescue Plan would provide billions of dollars for HCBS programs. Below are more details about the package. Check out the first blog to learn more.
- Increases the total dollars available for Medicaid HCBS, as states are required to maintain their current HCBS spending to qualify for the enhanced federal funds. Specifically, states have to maintain their level of HCBS spending as of April 1, 2021. The proposed 10 percentage point increase for HCBS is added to the state’s regular Medicaid matching rate (which ranges from 50% to 78% in FY 2022), as well as to other FMAP increases available to states, including the 6% percentage point increase for Community First Choice attendant care services, the 6.2% increase provided to address the COVID-19 public health emergency (PHE) under the Families First Coronavirus Response Act, any disaster recovery FMAP (available to states with a federally declared disaster and a certain amount of FMAP decline), and the 90% federal matching rate for Medicaid expansion adults under the ACA, as well as a proposed 5% in the regular matching rate for states newly adopting the ACA expansion provided in a separate section of the bill. The cumulative enhanced matching rate for Medicaid HCBS under the bill is capped at 95%.
- Estimated total Medicaid HCBS spending varies widely by state, ranging from $198 million dollars in Wyoming to nearly $22 billion in California. The additional $11.4 billion federal dollars from this FMAP increase is distributed proportional to the size of state HCBS programs, with California receiving nearly $2.2 billion additional federal dollars, Missouri $226 million and Wyoming receiving about $19.8 million additional federal dollars.
- States have a new option to provide community-based mobile crisis intervention services with 85% federal matching funds for the first 3 years. The additional funds must supplement, not supplant, the level of state spending for these services in the fiscal year before the first quarter that a state elects this option. Services must be otherwise covered by Medicaid and provided by a multidisciplinary team to enrollees experiencing a mental health or substance use disorder crisis outside of a hospital or other facility setting. These services generally do not have to be offered statewide, do not have to be comparable for all enrollees, and can restrict enrollees’ free choice of provider. The new option is available to states for 5 years, beginning April 1, 2022. The law also authorizes $15 million for state planning grants, to be awarded by the HHS Secretary as soon as practicable.
- Autistic individuals and their families have benefited from the economic impact payments provided by previous COVID-19 relief bills. However, those bills excluded dependents over the age of 16 from eligibility. The American Rescue Plan incorporates legislation to ensure that dependents over the age of 16 will qualify for $1,400 stimulus checks.
- The American Rescue Plan includes $3 billion in dedicated funding for Individuals with Disabilities Education Act (IDEA) programs.
- States may not use these funds to directly or indirectly reduce net tax revenue. This restriction will remain in place from March 3, 2021 until a state spends all remaining funds. If states violate this restriction, they must repay an equivalent amount of the federal aid.
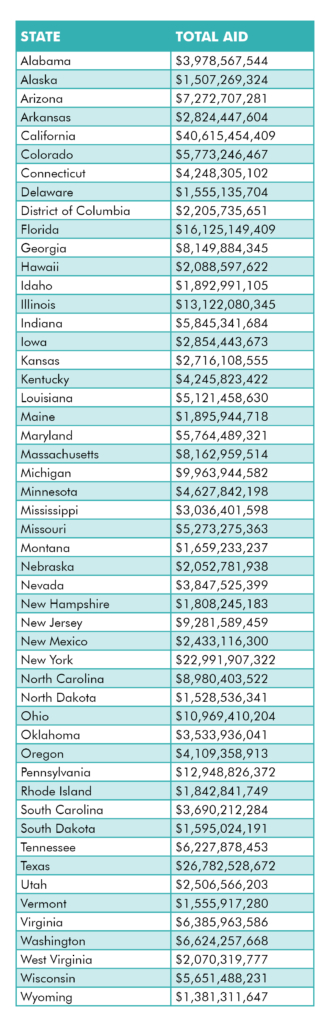
Use this chart to see how much funding your state will receive.